
By playing sports that required me to kick, I guess I should have seen a hip/groin related injury coming from a mile away. However, the way I ended up injuring my groin was squatting in a gym.
I had broken my ankle around 1o-weeks prior to this injury. I was in a cast, initially, for 4 weeks, and a moonboot for the following 6. The day of the injury, I was simply ecstatic to be finally free from the clutches of immobilization. Finally, I was “bulletproof” again.
I was in a squat rack, with the weight the same as it was pre-broken ankle. I remember my knees dipping in, and feeling a slight popping sensation through the front of my pelvis. It didn’t really hurt that much at the time, so I didn’t think I’d done anything serious.
I only realized things weren’t quite normal a few days later, when I was out playing social touch rugby with a few mates. I didn’t really have much pain, but I just couldn’t sprint. It was so strange. I could turn, jog, jump, lunge and dive. As the weeks rolled by, I started to notice that sitting was becoming sore the longer I sat for, and driving was near impossible for more than half an hour. I also had pain on coughing and sneezing, so I started to become quite concerned.
My physio also wasn’t sure what was going on, but had a thought that it could have been coming from my groin, as a GP had ruled out a hernia or anything like that as a diagnosis. The next step was to send me on to a Sports GP due to the length of time that had passed (about 3-4 months since injury at this point), and the with the rugby season approaching
rapidly.
The Sports GP diagnosed an Adductor Longus Tendinopathy. The Adductor Longus is one of the inner thigh muscles that make up the groin, with an origin through the front of the pubis (where the majority of my pain was felt). The most obvious test he used to prove the pain was muscular, was when he got me to lie in a sit-up position, and asked me to squeeze his fist between my knees. The pain was automatically reproduced, and I for the life of me could not generate any power between my knees.
What we did about it:
He started me on what is more commonly known as the Holmich Protocol. Per Holmich is a danish professor and researcher who has contributed a huge body of work to the understanding, treatment and prevention of groin injuries. He mostly works with football players, due to the increased incidence of groin injury in that population. It’s based around a series of exercises that are broken up into two modules, below are 3 of my favourite exercises from each module, but I will attach the full protocol in a link below. The exercises below are slightly modified so that you don’t need a lot of equipment to be able to complete them
Module 1


- Place a ball between your knees and squeeze as hard as you can for 10 seconds. Move the ball to between your feet and then squeeze for a further 10 seconds. Have 10 seconds rest and repeat 10 times.

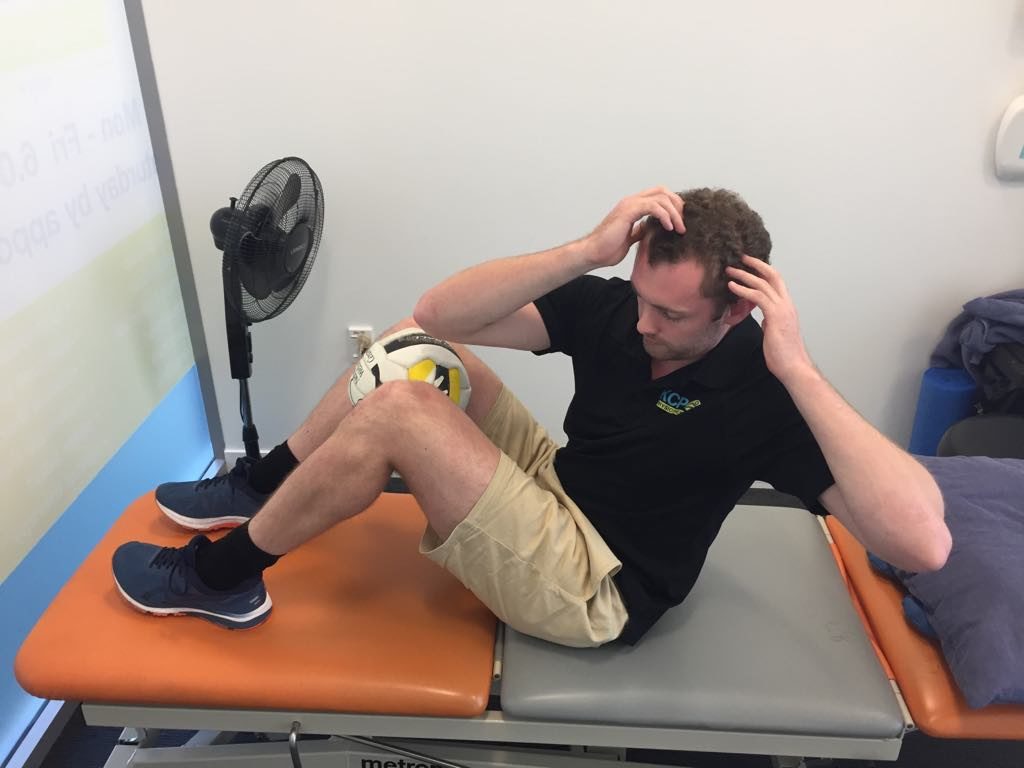

- Place a ball between your knees in a sit-up position. Perform a sit-up bringing your right elbow to your left knee, then a regular sit-up and then bringing your left elbow to your right knee. Repeat this 10 times, for a total of 5 rounds, with 1 minute rest between each round.


- Place a ball between your knees pre-situp position. Bring your knees up and perform a sit-up at the same time, making a “jack-knife” shape. repeat this for 5 sets of 10 reps, with 1 minute rest between each set.
Module 2


- Lie on you side and lift your top leg up as high as you can. Repeat this 10 times for a total of 5 sets. (This one is also a good primer exercise before sport/activity.)




- Using a Theraband tied under a stable table/chair and around one of your ankles, take 5 steps to the side increasing the tension through the band. Take 5 steps back towards the table, controlling the leg with smooth movement. Turn 180′ and repeat the 5 steps out and back. Rest for 1 minute between sets and complete 5 sets in total.


- Lie on your side with the sore leg up on a bench/chair. Lift your bottom leg up making a side bridge and hold for 10 seconds. Repeat this 5 times, for 3 sets in total. This is the most difficult exercise of the ones mentioned.
I’m not going to profess that at 19 years old I was the perfect patient, I probably got the exercises done two or three times a week rather than every day like the sports doctor recommended. Had I done them more often I probably would have got back to my previous level of sport a bit earlier, but for me the process was around four months to feeling like I could play rugby (sprinting and kicking) freely and without pain.
So if you’ve got a current groin injury, give the Holmich Protocol a go! Even if you got injured a while ago, the exercise programme can still help with your pain and function.
Teej
Effect of Holmich protocol exercise therapy on long-standing adductor-related groin pain in athletes: an objective evaluation https://bmjopensem.bmj.com/content/4/1/e000343?int_source=trendmd&int_medium=trendmd&int_campaign=trendmd